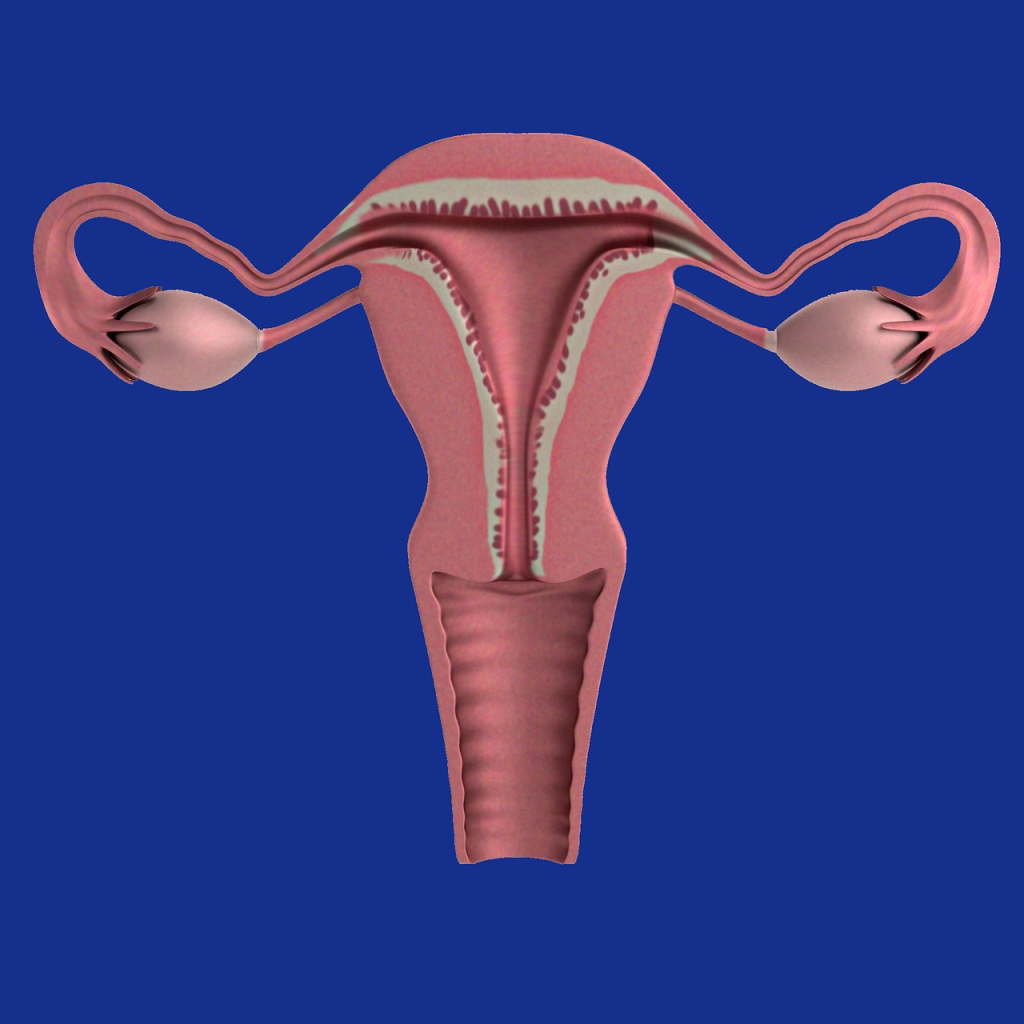
Description of Non-pregnant or non-gravid uterus
Uterus is a pear-shaped, hollow muscular organ which receives the insertion of two oviducts into its upper and outer angle. The uterus provides an environment for nourishment, growth and development of fetus during pregnancy till delivery.
Position: The uterus is located within the true pelvis above the vagina behind the bladder and in front of rectum in an anteverted and anteflexed manner.
Size: Measures 7.5cm long, 5cm wide, 2.5cm depth and 1.25cm thick in each wall. The uterus weighs about 60g.
Gross structure

The uterus is discribed in two parts which are the body and the cervix.
The body is the upper two-thirds of the uterus and this in turn consists of the following parts:
(a) Fundus: this is the broad rounded upper portion above the insertion of the tubes.
(b) Cavity: it is the hollow ‘D’ shaped area which has its base above and apex below and measures 5cm. Due to the flatness of the uterus, the anterior and posterior walls are in apposition.
(c) Cornua(horn): This is the lateral angle of the uterine body where fallopian tubes insert.
(d) Isthmus: This is the constricted or narrowed part which joins the body to the neck. Isthmus measures 7mm in length and is selected immediately above the internal is. Its function is to expand during the 2nd trimester of pregnancy to form lower uterine segment.
Cervix: This is the neck of the uterus. Cervix is spindled shaped portion of the uterus, which is described in two parts: the supravaginal and the intravaginal portions.
Macroscopic Structure
The walls of the uterus are mainly composed of plain muscle cells called the myometrium. The uterine cavity is lined by mucous membranes known as the endometrium and the peritoneum that covers the body the body of the uterus is known as perimetrium.
Endometrium:
This is the inner linning of the mucous membrane. The coporal endometrium undergoes series of changes from puberty to menopause(i.e. its appearance varies with each day of menstrual cycle). During menstruation, it is shed as far as the basal layer.
The cervical endometrium are of poor quality and do not undego any changes. The cervical endometrium is thrown into folds called arbo vitae (fern-like appearance)
Myometrium:
This is the plain muscular layer which forms the second middle coat of of the uterus. It forms ⅞th of the thickness of the uterine walls and its fibres are arranged in three patterns:
- Outer layer of longitudinal fibre: This passes over the fundus from the front to the back, begining and finishing at the level of internal os. Only few of its fibres extend or run into the cervix. It plays a crucial role in labour by contracting and retracting to shorten the upper uterine segment thereby pulling up and shortening of the cervix.
- The middle layer of oblique fibre: This is found mainly in the upper two-thirds of the uterus. These muscle fibres cross and inter-raced in every direction to form a figure of “8” pattern called the “Criss -cross” around the vascultures(blood vessels). Then some of the fibres extend into the cervix. When the placenta separate into the uterine wall at the end of labour, oblique fibres are capable of contracting and sealing off blood vessels to control haemorrhage, and hence, forestalling and preventing Postpartum haemorrhage — an action known as “nature’s living ligatures”.The oblique fibre of the myometrium is considered to be the strongest among other fibres.
- Inner circular fibre: This is thickly arranged around the cornua and in the lower uterine segment but very sparely in the uterine body. It is the weakest of the three layers but have an important role as they dilate and stretch during labour— to make the cervix more patent(10cm full dilatation) for delivery.
The Perimetrium
The outer part of peritoneum covers only the upper part of the uterus. It is reflected posteriorly to the rectum — forming the pouch of Douglas and also anteriorly to the bladder —forming the utero-vesical pouch.
Control of haemorrhage(action of living ligatures)
During third stage of labour, the oblique fibres which are arranged in the figure of ‘8’ patterns contract rhythmically. When these fibres contract, they ligate the arteries that pass via them thereby arresting bleeding.
In addition, the contractions of the oblique fibres result in occlusion of the blood vessels. When the vessels are ligated, the fibrins form at the cut- end of the vessels and clot forms which occlude the vessels — making the escape of blood to be controlled. That is haemostasis mechanism.
Anatomic relationships
Anteriorly: bladder, utero-vesical pouch, coils of intestines
Posteriorly: rectum and pouch of Douglas
Superiorly: coils of intestines
Inferiorly: vagina and the base of bladder
Laterally: Fallopian tubes, ovaries and broad ligaments
Supports of the uterus
The uterus is maintained or held in its position by 6 pairs of ligaments and individually by the pelvic floor muscles.
The supporting ligaments are:
- The two cardinal or transverse cervical ligaments: They run from the cervix to the side walls of the pelvis.
- The two uterosacral or sacrocervical liagments: These run from the cervix to the sacrum.
- The two pubocervical ligaments: These are weak ligaments that run from the cervix to pubic bone.
- The two round ligaments: They run from the cornua of the uterus to the groins.
- The two ovarian ligaments: These run from the cornua to the ovaries. They help to sustain the ovaries in their normal position.
- The two broad ligaments: These are two double fold of peritoneum passing laterally from the uterus to the side walls of the pelvis. They are folded over the fallopian tubes except the fimbriated end. Broad ligaments are not true ligaments of the uterus.
Blood, Nerve & Lymphatic Supply to Uterus
- Blood supply: uterine and ovarian arteries.
- Venous drainage: By corresponding veins
- Lymphatic drainage: The lymph drains into internal iliac glands
- Nerve supply: via Lee Frankenhaauser’s plexus.
Uterine Functions
- It takes part in menstrual cycle.
- It accommodates fetus and expels it at term during labour.
- It involutes following childbirth.
- It prepares bed for fertilized egg to implant.

Changes that occurs in the uterus during pregnancy
Position: By 12th weeks of pregnancy, the uterus rises out of the pelvis to become an abdominal organ. It is more vertical than anteverted and anteflexed.
Shape: As the uterus is increasing in size, its shape becomes modified. At the onset of pregnancy, it’s pear-shaped. But by the end of third month, it becomes globular. Between 12th and 36th weeks, it becomes ovoid as the fetus grows longer. By the end of the third month, the isthmus widens out to form the lower uterine segment.
Size: As the pregnancy advances, the uterus with 60g weight and 7.5cm long, 5cm wide and 2.5cm thick becomes 30cm long, 23cm wide and 20cm thick and weighs 900-1000g. The Isthmus increases from 7mm to 25mm in length.
Changes in myoctyes(uterine muscle cells)
The uterine muscle growth during pregnancy occurs in two ways which are:
Hypertrophy: The actual muscle cells enlarge, increasing ten times in length and five times in width.
Hyperplasia: New muscle cells appear and grow along side of the pre-existing muscle cells.
Other changes occurring during pregnancy are:
- Development of deciduae from endometrium. Hence, pregnant endometrium is known as Decidua
- There is increased vascularity during pregnancy.
- The ligaments which contain smooth muscle become thickened during pregnancy as a result of growth of muscle fibres.
- The liagments maintain their length of 2.5cm but are softer after the third month due to Increased vascularity and relaxing effects of progesterone and relaxin.
- The cervical gland secrets a mucous plug called operculum which occludes the cervical canal during pregnancy and prevents ascending infections.
Physiology of uterus during pregnancy
The uterus does not only enlarge remarkably to accommodate the growing fetus but also relaxes in order not to expel the fetus before term(uterus is intrinsically contractile). The growth and relaxation of uterine muscles are due to the hormones, oestrogen and progesterone respectively, both from corpus luteum and later from the placenta.
The uterus, however, is not completely relaxed. This is because from 8th weeks onwards, periodic waves of contractions pass via the uterus. This lasts only for one minute and reoccur at 5-10 minutes intervals. They are painless and women are unaware of their presence. These uterine contractions are known as “Braxton Hicks contractions”, “false labour” or “practice contraction” because they are simply preparing uterus for the role it would play during labour.
Towards the end of pregnancy, the contractions become stronger and more frequent and are responsible for taking up of the cervix(effacement) during the last month of pregnancy. They increase during labour and become true labour contractions, and the woman then experiences discomfort or pain.
The bottom line
The uterus otherwise known as womb, is a pear-shaped muscular organ of the female reproductive system which is suitated between the bladder anteriorly and the rectum posteriorly. It houses and nourishes fertilized egg (zygote) till delivery. That’s the uterus is the centre for implantation, gestation, menstruation and labour.
